What is Proton Beam Radiation Therapy?
Radiotherapy has been part of cancer treatment for decades. Most people have a general sense of what it involves. High-energy beams. Targeting a tumour. A course of treatment over several weeks.


Jump to:
Proton beam therapy sits within that, but it works slightly differently. It’s not a completely separate idea. It’s still radiotherapy. Just delivered in a more controlled way.
How Proton Beam Therapy Actually Works
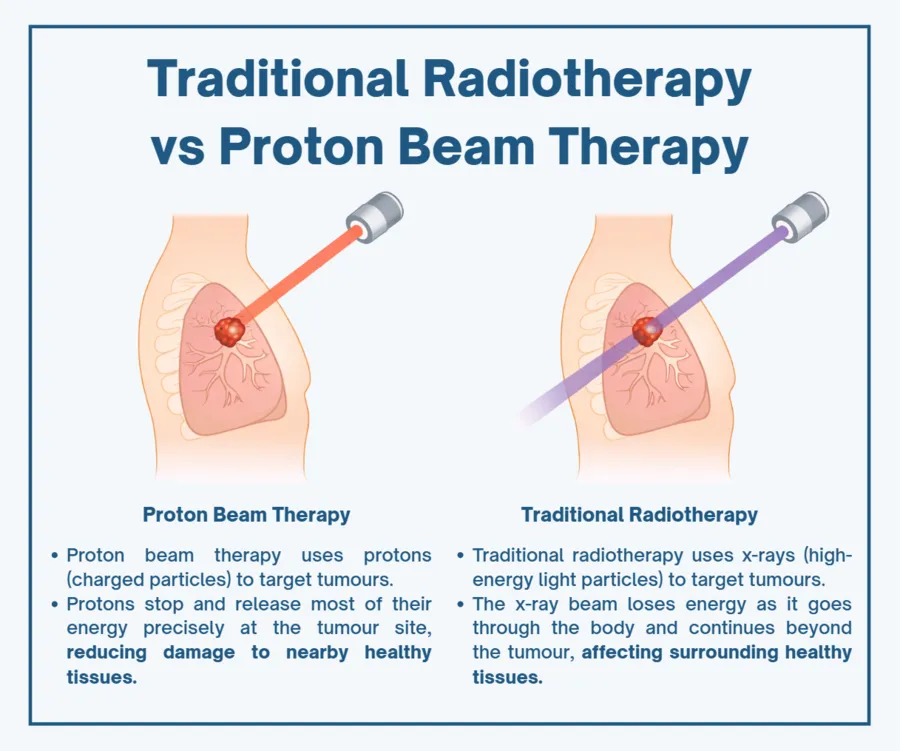
Traditional radiotherapy uses X-rays. They pass through the body, delivering radiation as they go. That works well, but it also means healthy tissue in front of and behind the tumour is exposed.
Proton beam therapy is different. Protons are charged particles. They can be directed to release most of their energy at a very specific depth, which is called the Bragg peak.
In simple terms, the radiation stops where it’s needed.
That changes things. It means less spill into surrounding tissue, particularly beyond the tumour.
If you’re looking at how this is used in practice, the approach to proton beam therapy focuses on that precision. Not just hitting the tumour, but limiting what sits around it from being affected unnecessarily.
Why That Precision Matters
Cancer treatment is always a balance. You want to treat the disease effectively, but not at the cost of long-term damage to healthy tissue that could have been avoided.
With standard radiotherapy, the outcomes can be very good. But there are situations where even small reductions in radiation to healthy tissue make a real difference.
Particularly when the tumour is close to something important - Healthy lung tissue; the spinal cord; the heart.
There’s also the question of cumulative exposure. If someone has already had radiotherapy before, you can’t always just repeat the same approach safely.
Proton therapy gives another option in those cases.
There’s some useful data around this. Studies have shown that proton therapy can reduce radiation dose to surrounding organs by up to 60% in certain tumour sites, depending on location and planning.
That doesn’t automatically make it the right choice for everyone. But it does expand what’s possible.
When Proton Beam Therapy is Usually Considered
It isn’t used for every cancer. And it shouldn’t be. Where it tends to come into its own is when precision really matters.
Brain tumours are a good example. Even small doses to the surrounding brain tissue can affect cognition over time. Reducing that exposure is not a small thing.
Spinal tumours are similar. The margin for error is narrow. You’re working very close to the spinal cord, which doesn’t tolerate radiation well.
Head and neck cancers also come up often. These areas are dense with structures that affect swallowing, speech, and taste. Standard radiotherapy can treat the cancer effectively, but side effects can be significant.
In children, the conversation is slightly different. Long-term effects matter more simply because of life expectancy. Proton therapy is often considered to reduce the risk of growth issues or secondary cancers later on.
The common thread is this. You’re trying to treat something difficult without creating a new problem alongside it.
How is Proton Beam Therapy Used in Lung Cancer?
Lung cancer sits slightly differently.
It is not a routine choice for every patient. Standard radiotherapy remains highly effective in many cases. But there are situations where the precision of proton therapy becomes more relevant.
This is usually when the tumour is close to critical structures such as the heart, oesophagus, or spinal cord. In those cases, even small reductions in radiation to surrounding tissue can make a meaningful difference.
There are also situations where patients have previously received radiotherapy. In that context, limiting additional exposure to already treated areas becomes important.
What this means in practice is that proton beam therapy is considered when the balance between treating the cancer effectively and protecting surrounding tissue becomes more difficult.
It is not about replacing standard radiotherapy. It is about expanding what can be done safely in more complex cases.
What Treatment Looks Like in Practice
From the outside, it doesn’t feel dramatically different from standard radiotherapy.
You attend a specialist centre. There’s planning beforehand, often quite detailed. Scans, positioning, and mapping the exact area to treat. That’s also where a lot of the personalised care comes in. The treatment isn’t generic. It’s shaped around the tumour, but also around the person.
Treatment itself is usually delivered over several sessions. Each one is relatively short.
The complexity sits behind the scenes. The physics, the planning, the calibration of the beam. That’s where most of the work happens.
From a patient’s point of view, it’s more about consistency. Turning up. Getting through the course of treatment. Managing any side effects along the way.
Are There Downsides?
It’s not a perfect solution. Nothing in oncology is.
Access is one of the main limitations. There are fewer centres offering proton therapy compared to standard radiotherapy.
It’s also more expensive. That has implications, depending on how treatment is being funded.
And clinically, it’s not always necessary. In many cases, conventional radiotherapy does the job very well without the added complexity.
So the question is rarely “is this better?”
It’s more, “Is this better for this particular situation?” That distinction matters.
Where it Fits in The Bigger Picture
Proton beam therapy isn’t a replacement for everything else. It sits alongside surgery, chemotherapy, immunotherapy, and standard radiotherapy.
Sometimes it’s the main treatment. Sometimes it’s part of a combined approach.
What’s changed over the past decade is the level of control we now have. The ability to tailor treatment more closely to the individual, rather than relying on a one-size approach.
That doesn’t make decisions easier. If anything, it adds more to think about.
But it does mean there are more options than there used to be.
About Dr James Wilson
Dr James Wilson is a London-based Consultant Clinical Oncologist specialising in lung cancer and advanced radiotherapy techniques. His work focuses on helping patients access clear, timely treatment plans without unnecessary delay, particularly when decisions feel complex or options seem limited. He is actively involved in discussions around improving cancer care pathways and ensuring patients are aware of all appropriate treatment options available to them.