Non-Small Cell vs Small Cell Lung Cancer: What’s the Difference?
When someone hears “lung cancer”, it sounds like one single thing. One diagnosis. One path.


Jump to:
In reality, it is not that simple.
There are two main types. Non-small cell lung cancer and small cell lung cancer. They behave differently. They grow differently. And they are treated differently. That distinction matters more than most people realise.
To be honest, understanding the type is one of the first steps in working out what happens next.
The two main types of lung cancer
Broadly speaking, lung cancer is divided into two categories under the microscope.
The simplest way to think about it is this:
-
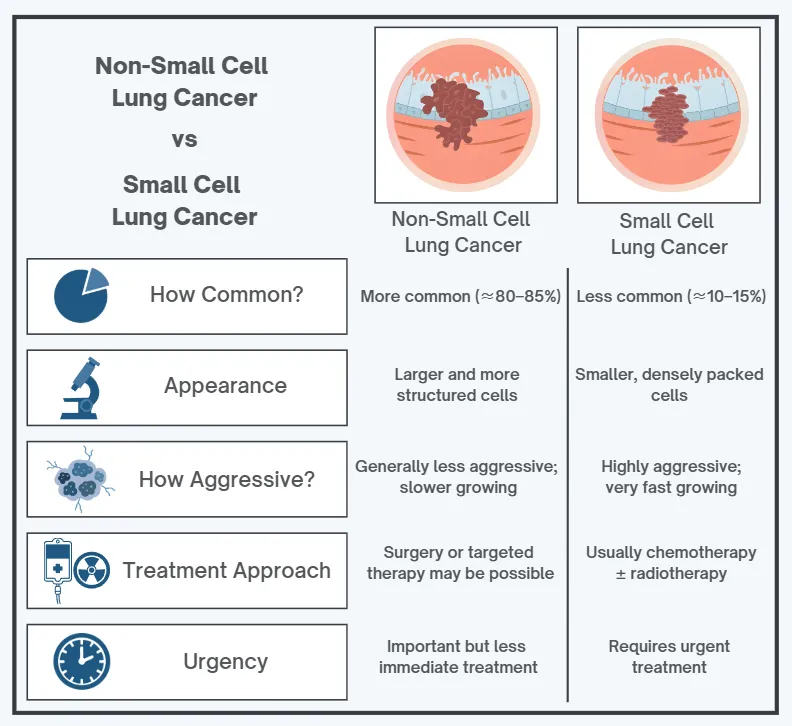
Non-small cell lung cancer (NSCLC) is more common and can develop more slowly.
-
Small cell lung cancer (SCLC) is less common and usually spreads more quickly.
That doesn’t mean one is “better” or “worse” in any neat way. It means they are different diseases, and we treat them differently.
In the UK, around 80–85% of lung cancers are NSCLC. SCLC makes up around 10–15%.
That split alone tells you something important. Most people we see are dealing with non-small cell disease.
But numbers only tell part of the story.
When we build a lung cancer treatment plan, the type of cancer is one of the first and most critical pieces of information. It influences whether surgery is appropriate, whether immunotherapy is an option, and how urgently treatment needs to begin.
So what actually separates them?
How the cells look under the microscope
The difference starts at a cellular level.
When a biopsy is taken, a pathologist examines the tissue under a microscope. Non-small cell lung cancer cells tend to be larger and more structured.
NSCLC is not a single entity. It includes:
-
Adenocarcinoma
-
Squamous cell carcinoma
-
Large cell carcinoma
These subtypes are defined by how the cells look and where they tend to arise within the lung. Adenocarcinoma, for example, often develops in the outer parts of the lung. Squamous cell carcinoma is more commonly linked to the central airways.
Importantly, many cases of NSCLC can now be tested for specific genetic mutations. In selected patients, this allows us to use targeted treatments rather than standard chemotherapy alone.
Small cell lung cancer looks very different under the microscope. The cells are smaller, densely packed, and divide rapidly. They appear uniform. Aggressive.
It is not just a technical distinction. That microscopic difference reflects how the cancer behaves in the body.
And that behaviour drives everything that follows.
Growth and spread
Small cell lung cancer is typically more aggressive. It tends to grow quickly and spread early, often to lymph nodes, the liver, bones, or the brain. By the time it is diagnosed, it has frequently moved beyond the lung itself.
That is not always the case. But often enough that we approach it with urgency.
Non-small cell lung cancer usually grows more slowly. It may remain confined to one part of the lung for longer. That can create a window where surgery or stereotactic ablative radiotherapy, known as SABR, is possible with curative intent.
This is why staging investigations are so important.
CT scans. PET-CT scans. MRI of the brain where appropriate. We are not just confirming a lung cancer diagnosis. We are trying to understand the full extent of the disease so that treatment is proportionate and precise.
It is tempting to think of lung cancer as one pathway. It really is not. The biology shapes the timeline.
Symptoms: why they can look the same
Non-small cell and small cell lung cancer can cause very similar symptoms, especially early on. That is because symptoms are often driven by where the tumour is located, not just what type it is.
Common symptoms include:
-
Persistent cough
-
Breathlessness
-
Chest discomfort
-
Coughing up blood
-
Recurrent chest infections
-
Unexplained weight loss and fatigue
Sometimes the first clue is a complication. Fluid around the lung, known as a pleural effusion, can cause sudden breathlessness. If breathing is worsening quickly, that needs prompt assessment.
Because small cell lung cancer spreads earlier, it may also present with symptoms related to other organs. Headaches or neurological changes from brain involvement. Bone pain. Occasionally, hormone-related syndromes.
The overlap in symptoms is one reason biopsy and proper pathological analysis are essential. We cannot reliably distinguish these cancers based on symptoms alone.
Treatment approach: why the type changes everything
The treatment pathway for lung cancer is built around the cell type and stage.
In early-stage non-small cell lung cancer, surgery or SABR may be offered with curative intent. In more advanced stages, treatment may involve chemotherapy, immunotherapy, targeted therapy, or a combination of these.
Molecular testing is now standard for many patients with advanced NSCLC. Identifying mutations such as EGFR or ALK can significantly alter the treatment approach.
In small cell lung cancer, treatment usually starts with chemotherapy combined with immunotherapy. Radiotherapy is often added in limited-stage disease. Surgery is uncommon because the cancer has often spread by the time it is diagnosed.
The aim may be cure in selected limited-stage cases, but more often it is long-term control or symptom relief.
This is why defining the diagnosis clearly at the outset matters. A biopsy is essential. Not just to confirm cancer, but to determine the exact subtype and allow full testing.
When we structure a personalised cancer care plan, the cell type, stage, molecular profile, and overall health of the patient all come together. It is not a one-size-fits-all process. It is a series of decisions made carefully and, ideally, promptly.
Prognosis: The honest answer is, it depends
People understandably want numbers. The reality is that outcomes depend on several things, including:
-
Stage at diagnosis
-
General health and lung function
-
Exact pathology and subtype
-
Molecular profile (particularly in NSCLC)
-
How well the cancer responds to first-line treatment
In general, earlier-stage NSCLC has the best chance of cure, often with surgery or SABR. SCLC is less commonly diagnosed at an early stage, which is one reason it can be more challenging overall.
But none of this is a reason to assume the worst. Treatments have moved on quickly, and many people are offered more options now than they would have been even a few years ago.
When to push for a faster review
If you’re waiting on a biopsy, waiting on staging scans, or you’ve been told a plan but it still doesn’t quite add up, you’re not being difficult by asking for clarity.
It’s completely reasonable to ask:
-
Do we know if this is NSCLC or SCLC yet?
-
Have we done the right biopsy to allow full testing?
-
Do we have staging confirmed (including PET-CT if appropriate)?
-
Is molecular testing being done (for NSCLC)?
-
What’s the aim of treatment: cure, long-term control, symptom relief?
If you feel stuck in limbo, a second opinion can often help confirm the diagnosis, speed up the pathway, and make sure nothing important has been missed.
About Dr. James Wilson
Dr. James Wilson is a consultant oncologist with expertise in lung cancer and advanced radiotherapy. Working full-time in private practice in Central London, he offers accurate diagnosis, comprehensive staging, and carefully structured treatment planning shaped by individual disease biology. For people navigating the decisions that follow a small cell or non-small cell diagnosis, that clarity and precision make all the difference.