How Is Lung Cancer Diagnosed?
If you’re worried about lung cancer, the wait for answers is often the hardest part. Not the tests themselves. It’s the not knowing what’s going on, what the plan is, and how long it’s all going to take.


Jump to:
The good news is that diagnosing lung cancer usually follows a clear, step-by-step pathway. Some people will need only a couple of tests. Others need a more detailed work-up, especially if we’re trying to confirm the type of lung cancer and whether it has spread.
When Do We Start Investigating?
We tend to begin with symptoms or an abnormal scan.
Common triggers include:
-
persistent cough
-
coughing up blood
-
unexplained shortness of breath
-
chest pain
-
unexpected weight loss
Occasionally, an abnormality is picked up incidentally on a chest X-ray done for something else. That happens more often than people think.
The first step is usually imaging. A chest X-ray may show a shadow. If it does, or if symptoms remain concerning, we move to a CT scan of the chest. A CT gives far more detail. It allows us to see the size, position, and characteristics of a lesion.
At this stage, we are not yet at a definitive answer. A CT can suggest cancer. It cannot prove it.
A proper lung cancer diagnosis requires tissue. That is the point at which we move from educated suspicion to certainty. The key is obtaining a biopsy safely and efficiently. And yes, it is often the waiting that feels the hardest.
Imaging in More Detail
Once a suspicious area is identified on CT, further imaging is usually required.
A PET-CT scan is commonly performed. This looks at metabolic activity. Cancer cells often use more glucose than normal tissue, so they “light up” on the scan. It helps us understand whether the abnormality is active and whether it has spread elsewhere in the body.
We may also arrange an MRI scan of the brain, particularly in certain types of lung cancer or if there are neurological symptoms. Lung cancer can spread to the brain. It is better to know early if it has.
Imaging gives us the map. But again, imaging alone is not a diagnosis.
The Role of Biopsy
This is the crucial step. A biopsy involves taking a small sample of tissue so that a pathologist can examine it under a microscope. It confirms whether cancer is present. It also tells us what type of lung cancer it is.
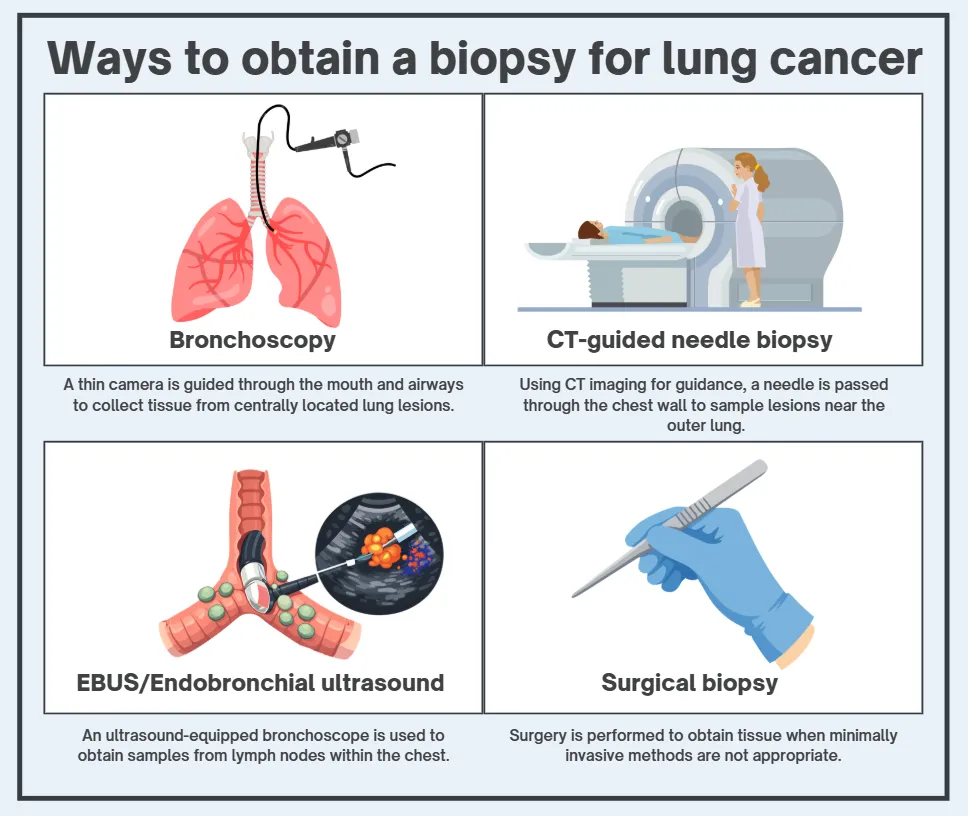
There are several ways to obtain a biopsy:
-
Bronchoscopy. A camera is passed through the mouth into the lungs to sample central lesions.
-
CT-guided needle biopsy. A needle is inserted through the chest wall into a peripheral lesion under CT guidance.
-
EBUS. Endobronchial ultrasound allows sampling of lymph nodes in the chest.
-
Occasionally, a surgical biopsy is required if less invasive approaches are not suitable.
The choice depends on the position of the tumour and the patient’s overall health. We balance accuracy with safety. Always.
To be honest, this is often the point where anxiety peaks. It feels more real once tissue is taken. That is understandable. But it is also the point where uncertainty begins to narrow.
Understanding the Type of Lung Cancer
Not all lung cancers are the same.
Broadly, we divide them into non-small cell lung cancer and small cell lung cancer. That distinction matters. Treatment pathways differ significantly.
Within non-small cell lung cancer, there are subtypes such as adenocarcinoma, squamous cell carcinoma, and less common variants. The pathology report gives us this information.
Modern diagnosis goes further. We now test tumour tissue for specific genetic mutations and molecular markers. These include alterations such as EGFR, ALK, ROS1, and others. They can determine eligibility for targeted therapies or immunotherapy.
I mean, this is where personalised lung cancer care has genuinely evolved. Ten or fifteen years ago, we did not have the same depth of molecular insight. Now, it is routine. And it matters enormously for treatment planning.
Staging the Cancer
Diagnosis is not just about confirming cancer. It is also about determining its stage.
Staging tells us how far the cancer has spread. We use the TNM system:
-
T for tumour size and local invasion
-
N for lymph node involvement
-
M for metastasis to distant organs
The combination determines whether the cancer is stage I, II, III, or IV.
Why does this matter? Because treatment decisions are based on the stage. Early-stage disease may be treated with surgery, sometimes followed by chemotherapy or radiotherapy. More advanced stages may require systemic treatment, such as chemotherapy, immunotherapy, or targeted therapy.
It is bloody hard hearing the word “stage”. Patients often assume it immediately translates into prognosis. It does not always. The stage is part of the picture. It is not the whole story.
How Long Does Diagnosis Take?
People often want a clear timeline.
In an ideal setting, the process from suspicious scan to confirmed diagnosis and staging should take a couple of weeks. Sometimes faster. Delays can occur, particularly if multiple tests are required or if biopsy samples need further molecular analysis.
One of the frustrations I see repeatedly is system delay. Waiting for scans. Waiting for reports and authorisations. I wish this part were faster. We all do.
In private practice, we try to compress that timelin. Not to rush decisions, but to avoid unnecessary pauses to get you to treatment as quickly as possible. Clarity reduces anxiety even when the news is difficult.
What Happens After Diagnosis?
Once diagnosis and staging are complete, the case is usually discussed in a multidisciplinary team meeting. Surgeons, oncologists, radiologists, pathologists, and specialist nurses review the findings together.
This is important. No single clinician makes decisions in isolation. We look at the imaging, the pathology, the patient’s overall health, and their preferences.
Then we sit down and talk it through. Properly.
You know, it is easy to focus on the technical side of diagnosis. Scans. Biopsies. Molecular markers. But what patients remember is often the conversation. The moment when uncertainty becomes defined.
Diagnosis is not just a clinical event. It is a turning point. Our job is to make that turning point as clear, honest, and well-supported as possible.
About Dr. James Wislon
Dr. James Wilson is a consultant oncologist with expertise in lung cancer and advanced radiotherapy. Working full-time in private practice in Central London, he offers prompt diagnosis, transparent plans, and reassuring, actionable guidance in time‑critical situations.