Expert Thymoma Treatment in London: Clarity When You Need It Most
When you've been diagnosed with thymoma or thymic carcinoma, finding a specialist who truly understands this rare cancer can feel impossible. You deserve clear answers, not vague explanations. You need a consultant oncologist who has treated thymoma many times before, not someone seeing their first case.
I'm Dr James Wilson, a consultant oncologist specialising in thymoma and thymic epithelial tumors. I provide rapid access to the best treatment for thymoma at leading London hospitals, with a multidisciplinary team who know exactly what to do.
Why Patients Choose Dr James Wilson for Thymoma Care
When you need a true specialist in rare thymic tumours, not a generalist
Thymoma Specialist
Years treating rare thymic tumours with proven outcomes
Proton Beam Therapy Access
Precision radiation that protects your heart and lungs
Multidisciplinary Team Coordination
Leading expert surgeons, oncologists, and specialists working together for you
Fast Access
Appointments within days, not weeks. Video consultations available UK-wide
Dr James Wilson discusses specialist thymoma treatment with patient Lesley Garrett on ITV's This Morning
I appeared on ITV's This Morning to discuss thymoma treatment with my patient, renowned opera singer Dame Lesley Garrett CBE. Lesley's case demonstrates what specialist thymoma care can achieve: complete tumour control with minimal impact on her extraordinary vocal ability.
What started as an incidental finding during breast screening revealed a thymoma on Lesley's thymus gland. When she noticed subtle changes in her breathing and vocal range, changes that only a professional singer might detect, we knew the tumour needed to be addressed.
The results speak for themselves: Lesley was singing the day after surgery and performing on stage within three months. Her voice remained perfect throughout her treatment and recovery.
How We Deliver Expert Thymoma Treatment in London
You don't have time for generalists. Thymoma requires someone who understands the nuances of this rare cancer, from diagnosis through to long-term follow-up.
What makes our thymoma care different:
Genuine Expertise in Rare Thymus Cancer I specialise in thymoma and thymic carcinoma. This isn't something I see occasionally. I work with patients facing this diagnosis regularly, and I understand the unique challenges of thymic epithelial tumors, including their association with autoimmune conditions like myasthenia gravis.
Rapid Access Without NHS Delays Private thymoma treatment London means you can see me within days, not weeks. Your scans are reviewed the same day, your treatment plan is created quickly, and you start therapy without unnecessary waiting.
Coordinated Multidisciplinary Care Thymoma treatment requires collaboration between thoracic surgeons, radiation oncologists, and specialists who understand autoimmune complications. I coordinate your entire care team so you never feel like you're managing this alone.
Access to Advanced Treatment Options From intensity-modulated radiation therapy (IMRT) to proton beam therapy, stereotactic radiotherapy to the latest targeted therapy options, I ensure you have access to the most appropriate treatment for your specific situation.
Proton Beam Therapy Access I'm one of the few UK oncologists offering proton beam therapy for thymoma. This cutting-edge treatment delivers radiation with unprecedented precision, dramatically reducing dose to your heart and lungs while maintaining excellent tumour control.
Our Reviews
What people are saying
“I had the privilege to have Dr Wilson as my consultant in treating my recent medical issue. His technical expertise is top class, but, of equal importance to me is that he has excellent communication skills, he is very easily approachable and sensitive to the patient‘s needs and makes complicated medical terms easily understood and followed by his patients. He has succeeded in having a very capable team as his assistants, which is also a significant virtue in a consultant ‘s role.”
Mrs YY
Understanding Thymoma and Thymic Carcinoma
What is Thymoma?
Thymoma is a rare cancer that develops in the thymus gland, a small organ located in your upper chest behind your breastbone (sternum). The thymus gland plays a vital role in your immune system, particularly during early development.
While all thymomas have the potential to behave like cancer, they differ from many other cancers in important ways. Thymoma typically grows more slowly and responds well to treatment when managed by specialists who understand this disease.
Key facts about thymoma:
Thymomas are rare, affecting approximately 1.5 per million people annually in the UK
They can occur at any age but are most common between 40 and 60
About 30-40% of thymoma patients also have myasthenia gravis, an autoimmune condition
Thymus gland cancer has a better prognosis than many other cancer types when treated appropriately
Thymoma Symptoms: What to Watch For
Many patients with thymoma have no symptoms initially. The tumour is often discovered during a chest X-ray or CT scan for another reason. When symptoms do occur, they may include:
Persistent cough that doesn't improve
Chest pain or pressure
Shortness of breath or difficulty breathing
Problems swallowing
Muscle weakness (particularly if you have myasthenia gravis thymoma)
Swelling in the face, neck, or upper body
If you're experiencing these symptoms and have concerns about thymus cancer, getting an expert opinion quickly is essential.
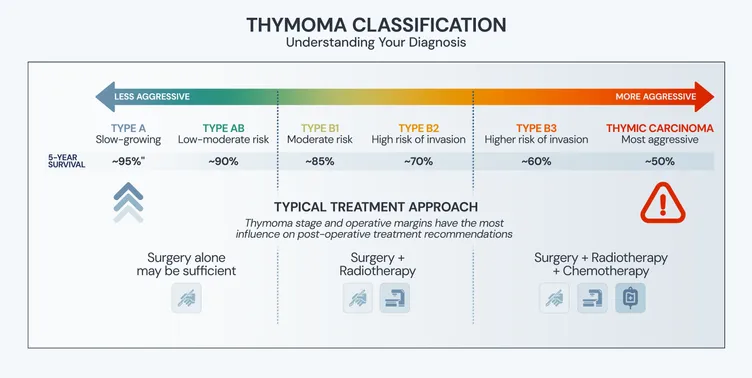
Types of Thymoma: Understanding Your Diagnosis
Thymomas are classified by the World Health Organisation (WHO) based on how the cancer cells look under a microscope:
Type A and AB thymoma: Generally less aggressive
Type B1, B2, and B3 thymoma: Increasingly aggressive behaviour
Thymic carcinoma: The most aggressive form of thymic epithelial tumors
This classification, alongside staging, determines the best treatment for thymoma in your specific case.
Thymic carcinoma is a more aggressive of thymic tumour (sometimes called thymus cancer or malignant thymoma) with clear cancerous features. It behaves more aggressively than the thymoma cancer type, growing quickly and often spreading to other parts of the body. Treatment typically requires a more intensive approach and use of a different treatment option.
Collectively, thymomas and thymic carcinomas are known as thymic epithelial tumours, representing the most common tumours of the anterior mediastinum (the front part of the chest between the lungs).
Your Thymoma treatment plan
Step 1
Fast Initial Consultation
Step 2
Test Results & Review
Step 3
Personalised Treatment Plan
Step 4
Targeted Cancer Treatment
Step 5
Follow-Up Care and Support
What tests do you need to make a diagnosis of thymoma?
If a thymoma or thymic cancer is suspected, your doctor will likely recommend:
CT scan
The primary imaging method for suspected thymoma, providing detailed information about the tumour's size, location, and potential invasion
MRI scan
Sometimes used to complement CT, particularly to distinguish thymic tumours from other masses
FDG-PET/CT (PET scan)
Not everybody with thymoma needs a PET scan. I will discuss whether we need to do a PET scan with you based on your personal situation
Blood tests for thymoma and associated conditions
Including tests for antibody levels and also autoantibodies associated with myasthenia gravis, and other blood tests to rule out other conditions which can look like thymoma on scans (e.g. germ cell tumours)
Biopsy
A biopsy is not usually needed if the scans have the appearance of thymoma and if the tumour is thought to be operable. In some cases, particularly in advanced thymoma, tissue sampling may be necessary to confirm the diagnosis.
Private Thymoma Treatment London: Your Options Explained
The goal of thymoma treatment is to remove or control the tumor while preserving your quality of life. Treatment depends on several factors including the stage of disease, tumor type, and whether you have conditions like myasthenia gravis.
Surgical Resection: The Foundation of Thymoma Treatment
Surgery remains the cornerstone of treatment for most patients. Complete surgical resection of the tumor, including removal of the entire thymus gland (thymectomy), offers the highest chance of long-term control.
For early-stage thymoma, surgery alone may be sufficient. Five-year survival rates for completely resected stage I thymoma typically exceed 80%.
When is surgery recommended?
Localised thymoma that can be completely removed
Invasive thymoma where surgical resection is technically feasible
As part of treatment for myasthenia and thymoma
Radiation Therapy for Thymoma
Radiotherapy plays an important role in many cases, particularly for:
Reducing recurrence risk after surgery (advanced thymoma or incomplete resection)
Treating recurrent thymoma
Managing inoperable disease
Advanced Radiation Techniques I Use:
Intensity-Modulated Radiation Therapy (IMRT) IMRT allows precise targeting of the tumor while protecting your heart, lungs, and other critical structures. This precision is essential given the location of the thymus gland in your chest.
Proton Beam Therapy For selected patients, proton beam therapy offers even greater precision than standard radiation therapy. This can significantly reduce long-term side effects, particularly important for younger patients or those with other health considerations.
Stereotactic Radiotherapy (SABR or SBRT) For small, well-defined areas of disease, stereotactic techniques deliver highly focused radiation in fewer treatment sessions.
Chemotherapy for Thymoma and Thymic Carcinoma
Chemotherapy may be recommended for:
Advanced thymoma that cannot be completely removed
Thymic carcinoma
Recurrent disease that has spread
Before surgery to shrink large tumors
Standard treatment regimens often include drugs like cyclophosphamide, cisplatin and doxorubicin, combined with other agents. The specific combination depends on your tumour type and overall health.
Targeted Therapy and Clinical Trials
For advanced or recurrent disease, newer treatment options are emerging:
Targeted therapy that attacks specific molecular features of cancer cells
Immunotherapy approaches (though these are used in the treatment of thymic carcinoma, but not really for thymoma - as it isn't very effective and also due to immune system complications)
Clinical trials investigating novel drugs and treatment combinations
As a specialist in rare cancer, I stay current with the latest research and can help determine if a clinical trial might be appropriate for you.
What are the benefits of proton beam therapy for thymoma?
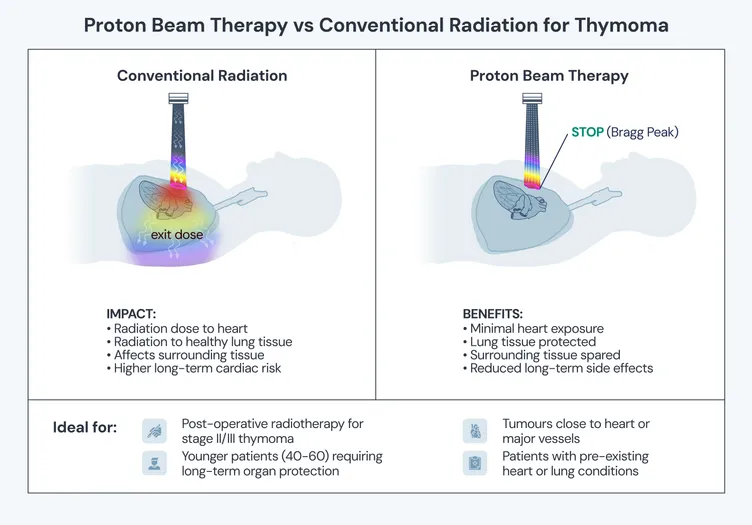
Proton Beam Therapy for Thymoma: Advanced Precision When Location Matters
The location of thymoma makes treatment challenging. Your thymus gland sits directly behind your breastbone, surrounded by your heart, lungs, and major blood vessels. Traditional radiation therapy must navigate this delicate area, and even with advanced IMRT, some radiation dose reaches these critical structures.
Proton beam therapy changes this equation entirely. I'm one of the few oncologists in the UK offering proton beam therapy for thymoma, giving my patients access to the most precise radiation treatment available.
What Makes Proton Beam Therapy Different?
Unlike conventional radiation (which continues through your body, affecting tissue beyond the tumor), protons stop precisely at the tumor target. This "Bragg peak" effect means:
Dramatically reduced radiation to your heart - protecting long-term cardiac function
Minimal lung exposure - reducing risk of radiation pneumonitis
Lower dose to surrounding tissue - fewer acute and long-term side effects
Same tumor control as conventional radiation - with significantly better safety profile
For thymoma patients, this precision is transformative. Because thymoma often affects younger patients (40-60 years old) who may live for decades after treatment, protecting healthy tissue from radiation damage has profound long-term implications.
When is Proton Beam Therapy Recommended for Thymoma?
I consider proton beam therapy for this cancer type in the following settings:
Post-operative radiotherapy - particularly for stage II, III, or invasive thymoma where the tumor was close to your heart or major vessels
Younger patients - where long-term cardiac and pulmonary protection is crucial
Patients with pre-existing heart or lung conditions - where additional radiation risk must be minimized
Recurrent thymoma near critical structures - where re-irradiation is needed
Large tumors requiring higher radiation doses - where proton precision offers maximum safety
Access to Proton Beam Therapy in London for thymoma
As a consultant Clinical oncologist (radiation oncologist) with access to the UK's leading proton beam therapy centres, I can arrange this treatment for appropriate patients. The technology is available at specialist facilities in London and the Southeast, and I coordinate the entire process.
Not every patient needs proton therapy - IMRT is highly effective for many cases. But when your clinical situation would benefit from protons, I am one of a small number of doctors who can ensure you have access to this treatment option.
What Proton Beam Treatment Involves
Proton beam therapy is delivered similarly to conventional radiotherapy:
Typically 25-30 treatment sessions over 5-6 weeks
Each session takes about 30-40 minutes (though much of this is setup)
Non-invasive and painless
Outpatient treatment - you can maintain your normal routine
The key difference is invisible to you but profound in its impact: the radiation stops exactly where it should, protecting the organs that keep you healthy for years to come.
Wherever you are in the world, we can support in you coming to London for this high-precision treatment for thymoma.
Who needs post-operative treatment for thymoma
After your operation to remove the thymoma, we'll discuss the details of your case. We'll review:
The stage of thymoma
The type (or grade) of thymoma
Whether the operation removed all of the thymoma or not
How close the thymoma was the the edge of the tissue that was removed - if there is evidence of thymoma cells right at the edge (the 'resection margin') it's important we know this.
I'll then make a recommendation as to whether further treatment is required or not.
Thymoma and Myasthenia Gravis: Coordinated Care
The relationship between thymoma and myasthenia gravis requires specialised management. Approximately 30-40% of thymoma patients develop myasthenia gravis, while 10-15% of myasthenia gravis patients have a thymoma.
What is myasthenia gravis? Myasthenia gravis is an autoimmune condition causing muscle weakness, particularly affecting your eyes, face, throat, and limbs. In thymoma patients, the abnormal thymus tissue can trigger production of antibodies that attack your neuromuscular junctions.
Managing both conditions:
Surgical resection of the thymoma often improves myasthenia symptoms
Medications like acetylcholinesterase inhibitors and immunosuppressants (including prednisone) manage ongoing muscle weakness
Close collaboration with neurology specialists ensures optimal care
Careful monitoring during and after cancer treatment
If you have myasthenia and thymoma, your treatment plan must address both conditions simultaneously. This requires experience and coordination across specialties.
What to Expect: Your Thymoma Treatment Journey
Step 1: Fast Initial Consultation
Your first consultation can happen within days. We'll discuss:
Your diagnosis and what it means
Your symptoms and how they're affecting you
Your concerns and questions
Initial thoughts on the best treatment approach
Many patients appreciate video consultations initially, particularly if travelling to London is difficult. This allows us to begin planning your care immediately.
Step 2: Comprehensive Diagnostic Review
I'll review all your imaging (CT scans, PET scans, MRI) and pathology results. If additional tests are needed, I'll arrange them quickly. This includes:
Confirming your WHO classification (Type A, AB, B1, B2, B3, or thymic carcinoma)
Accurate staging to understand disease extent
Assessment of lymph nodes and potential spread to the pleura or other structures
Evaluation for myasthenia gravis if not already diagnosed
Step 3: Multidisciplinary Team Discussion
Your case is presented to our specialist team including:
Thoracic surgeons experienced in thymectomy
Radiation oncologists
Medical oncologists
Specialist radiologists
Pathologists
Neurologists
Respiratory physicians
This ensures every perspective is considered and you receive truly coordinated care.
Step 4: Personalised Treatment Plan
You'll receive a clear, written treatment plan explaining:
Recommended treatment approach and why
Expected timeline
What to expect during treatment
Potential side effects and how we'll manage them
Prognosis and long-term outlook
No medical jargon without explanation. Just clear cancer information you can understand and share with your family.
Step 5: Treatment Delivery and Ongoing Support
Treatment takes place at world-class London hospitals with the most advanced technology. Throughout your care:
The exact cause of thymoma isn't fully understood. Experts believe it results from abnormal growth of cells in the thymus gland. Genetic mutations in tissue DNA may play a role, leading to changes in cell growth and causing abnormalities.
It's also common to have an autoimmune condition alongside thymoma, such as myasthenia gravis, which causes widespread muscle weakness.
How is thymoma diagnosed?
Diagnosis typically involves imaging studies such as chest X-rays and CT scans. MRI and PET scans are sometimes used too. A biopsy of the tumour tissue isn't always necessary but may be used to confirm the diagnosis and determine the WHO classification type. Some patients are diagnosed incidentally when having scans for other reasons.
How can I prevent thymoma?
Since the cause of thymoma isn’t entirely known, there’s no obvious way to prevent it. However, leading a healthy lifestyle and avoiding smoking may reduce your risk of thymomas and cancer generally.
Are all thymomas cancerous?
Yes, all thymomas are considered to have malignant potential, meaning they can invade surrounding structures and, in some cases, spread to distant sites. However, thymomas behave very differently from many other cancers. They typically grow more slowly and have a better prognosis when treated appropriately.
The WHO classification and staging system provide more accurate ways to describe the aggressiveness and extent of your thymoma.
Can thymoma be cured?
Many patients with early-stage thymoma can be cured, particularly when the tumor is completely removed with surgery. Five-year survival rates for stage I thymoma exceeds 90% with appropriate treatment.
For more advanced disease, long-term control is often achievable. Even recurrent thymoma can be managed for many years with the right approach.
Is a thymoma always cancer?
All thymomas have the potential to behave like cancer, but not all are equally aggressive. Type A and AB thymomas are generally less aggressive, while type B2, B3, and thymic carcinoma are more likely to invade local tissue or spread to lymph nodes and other areas.
The key is getting expert assessment and treatment from someone who specialises in these rare tumors.
Can a thymoma grow back?
Recurrent thymoma can occur, even years after successful initial treatment. This is why long-term follow-up is essential. The risk of recurrence depends on:
Initial stage and WHO type
Completeness of surgical resection
Whether radiotherapy was used
When recurrence does happen, treatment options include surgery (if technically feasible), radiation therapy, systemic therapy, or clinical trials.
Does everybody with thymoma need radiotherapy?
No, not every patient requires radiation therapy. The need for radiotherapy depends on:
Stage of the disease
Completeness of surgical resection
Histological subtype (WHO classification)
For completely resected stage I thymoma, radiotherapy is generally not recommended. For stage II, the decision depends on tumour type and invasion extent. For stage III and IV thymoma, post-operative radiotherapy is typically recommended due to higher recurrence risk.
Should I have proton beam therapy for my thymoma?
Proton beam therapy offers significant advantages for many thymoma patients, particularly those with tumors close to the heart or major vessels, younger patients where long-term side effect reduction matters most, or those requiring re-irradiation for recurrent disease.
The decision depends on your specific tumour location, stage, surgical outcome, and individual circumstances. During consultation, I'll review your imaging and discuss whether proton therapy would benefit you specifically.
What are the treatment options for recurrent thymoma?
When thymoma recurs after initial treatment, several options may be considered:
Surgery: If the recurrence is localised and technically resectable
Radiation therapy: Particularly if not used previously or for small, well-defined recurrences
Systemic therapy: Chemotherapy or targeted agents for widespread recurrence
Clinical trials: Investigating novel therapies
Many patients with recurrent thymoma can achieve meaningful disease control, sometimes for many years, through one or more of these approaches. The prognosis for recurrent disease is generally more favourable than for many other recurrent cancers.
How common is thymoma?
Thymoma is a rare cancer, affecting approximately 1.5 per million people annually. Because it's rare, many general oncologists have limited experience treating it. This makes finding a specialist particularly important.
What is the life expectancy for thymoma?
Prognosis varies significantly based on stage and type:
Stage I: 5-year survival often exceeds 90%
Stage II: 5-year survival typically 70-90%
Stage III: 5-year survival around 50-70%
Stage IV: 5-year survival approximately 30-50%
These are general figures. Your individual prognosis depends on many factors including your specific tumor type, how completely it can be removed, your overall health, and response to treatment.
What is the relationship between thymoma and myasthenia gravis?
Approximately 30-40% of thymoma patients develop myasthenia gravis. Conversely, about 10-15% of patients with myasthenia gravis will have a thymoma.
For patients with both conditions, treating the thymoma is essential, but specific management of the myasthenia gravis is also necessary. This typically includes medications and close collaboration between oncologists and neurologists.
What are the different types of thymoma?
Thymomas are classified by the World Health Organisation (WHO) system:
Type A: Generally the least aggressive
Type AB: Low to moderate risk
Type B1: Moderate risk
Type B2: Higher risk of invasion and spread
Type B3: Higher risk still
Thymic carcinoma: The most aggressive thymic epithelial tumor
This classification influences treatment decisions including surgical approach, whether to recommend post-operative radiation therapy, and need for chemotherapy or targeted therapy.
Is type B2 thymoma malignant?
Yes, type B2 thymoma is considered malignant and has a higher risk of invasive behaviour compared to types A, AB, or B1. Type B2 thymomas are more likely to invade through the tumour capsule and may require more aggressive treatment including surgery followed by radiotherapy.
Is type B3 thymoma malignant?
Yes, type B3 thymoma is malignant and among the more aggressive thymoma types, though still less aggressive than thymic carcinoma. Type B3 tumours often require multimodal treatment including surgical resection, radiation therapy, and sometimes chemotherapy.
What are the treatment options for recurrent thymoma?
When thymoma recurs after initial treatment, several options may be considered:
Surgery: If the recurrence is localised and technically resectable
Radiation therapy: Particularly if not used previously or for small, well-defined recurrences
Systemic therapy: Chemotherapy or targeted agents for widespread recurrence
Clinical trials: Investigating novel therapies
Many patients with recurrent thymoma achieve meaningful disease control, sometimes for many years.
Why London for Thymoma Treatment UK?
London is home to world-leading cancer centres with the most advanced treatment technology available anywhere in the world. Patients travel from across the UK and internationally for thymoma treatment in London because of:
Access to Cutting-Edge Technology
Latest generation linear accelerators for IMRT
Proton beam therapy facilities
MR-Linac for real-time image-guided radiotherapy
CyberKnife for stereotactic treatment
Multidisciplinary Expertise Leading thoracic surgeons, radiation oncologists, medical oncologists, and support specialists all working together in dedicated tumour boards.
Research and Clinical Trials Access to the latest clinical trials and experimental therapies through connections with institutions like the National Cancer Institute network.
My Hospital Affiliations: I treat patients at several prestigious London hospitals including:
The Cromwell Hospital
The London Clinic
LOC - Harley Street
LOC - Sydney Street
All of these facilities offer exceptional care with the latest treatment options for rare cancer.
For Patients Travelling to London: I can assist in arranging comfortable, convenient accommodation near my practices. Many of my patients live outside London or the UK, and we make the process as smooth as possible.
Video Consultations for Patients Across the UK
You don't need to travel to London for your first appointment. I offer video consultations to:
Provide rapid initial assessment
Review your diagnosis and scans
Develop a personalised treatment plan
Answer your questions face-to-face
This is particularly valuable for patients in Scotland, Wales, Northern Ireland, or other parts of England who want expert thymoma care but face travel difficulties.
Once your plan is established, treatment can often be delivered efficiently with minimal trips to London.
Take the Next Step: Book Your Thymoma Consultation
You've found a specialist who understands thymoma. Someone who has treated this rare cancer many times. Someone who can give you clarity, not confusion.
What happens when you contact us:
You'll speak with my team within 24 hours
We'll arrange a consultation (in-person or video) within a day or two
You'll get clear answers and a path forward
Your treatment can begin without unnecessary delay
You're welcome to:
Request a consultation to discuss your diagnosis
Ask questions about treatment options
Get a second opinion on your current plan
Discuss whether private treatment is right for you